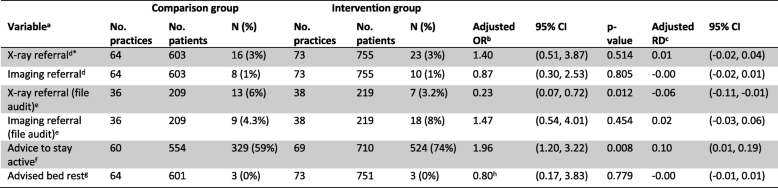
- *Primary outcome
- aX-ray referral was coded ‘Yes’ if the clinician ticked either “Lumbosacral plain X-ray” or “Full spine pain X-ray” at any of the patient consultations over the two week data collection period. Imaging referral was coded ‘Yes’ if the clinician ticked “Lumbar CT scan”, “Lumbar MRI”, or “Bone Scan” at any of the patient consultations over the two week data collection period. Advice to stay active is coded ‘Yes’ if the clinician ticks “Advice to stay active” at any of the patient consultations over the two week data collection period. Advised bed rest is coded ‘Yes’ if the clinician indicated “Bed rest” for greater than 2 days at any of the patient consultations over the 2 week data collection period
- bAdjusted effects from models fitted using generalised estimating equations analysis with exchangeable correlation (unless otherwise noted) structure and robust variance estimation to allow for clustering within practices. OR = odds ratio
- cRD risk difference. RD calculated from marginal probabilities. Confidence intervals were calculated using a pairwise comparison of margins after fitting a GEE model using Stata, allowing for clustering of observations within practices.
- dX-ray referral and imaging referral outcomes were only adjusted for the stratification variables, professional group (physiotherapist/chiropractor) and location of practice (urban/rural) due to high rates of adherence (resulting in low event rates)
- eAdjusted for: stratification variables (professional group, location of practice), patient level (age, sex, LBP compensation), clinician level (age, Gonstead practitioner, years in practice, special interest in LBP, postgraduate training, baseline intention (X-ray or imaging referral, as appropriate), and practice level (bulk billing, X-ray on site, compensable patients, number of clinicians in the practice). The pre-specified confounding variables ‘number visits for this episode of acute LBP’ and ‘≥ 1 x-ray LBP previous 12 mths’ were not adjusted for (see Additional file 1)
- fAdjusted for: stratification variables (professional group, location of practice), patient level (age, low back pain compensation, number of patient visits in the data collection period, exposure period, length of time with acute low back pain), clinician level (age, Gonstead practitioner, years in practice, special interest in low back pain, postgraduate training, baseline intention advice to stay active), and practice level (number of clinicians in the practice) (Fig. 2 of the trial protocol [22])
- gAdvised bed rest outcome is unadjusted for the stratification variables and pre-specified confounders due to a limited number of events
- hModelled with an independent correlation structure
